MRD (Minimal/Measurable Residual Disease) testing solves exactly this blind spot. By detecting traces of cancer DNA at sensitivities reaching 1 cancer cell in 1 million normal cells, MRD assays reveal disease persistence weeks or months before conventional methods catch up. This article explains what MRD testing is, how it works, which cancers benefit most, and why the quality of upstream lab processes—particularly cfDNA extraction—directly determines whether your results are accurate or dangerously misleading.
Key Takeaways
- MRD testing detects circulating tumor DNA (ctDNA) at sensitivities of 10⁻⁵ to 10⁻⁶, identifying residual cancer before imaging or symptoms appear
- Guideline-recommended for blood cancers (ALL, AML, CML, multiple myeloma); increasingly validated in solid tumors like colorectal and breast cancer
- Tumor-informed assays achieve 88% sensitivity in serial monitoring versus 59% for tumor-agnostic assays
- MRD-negative status reduces progression risk by 60% versus MRD-positive patients
- MRD-negative detection carries a median 5.5–7.9 month lead time over conventional imaging
- cfDNA input below 2 ng cuts assay sensitivity nearly in half — from 82.6% to 46.7%
What Is MRD Testing?
MRD (Minimal or Measurable Residual Disease) refers to the small number of cancer-derived molecular markers—primarily circulating tumor DNA (ctDNA)—that remain detectable in a patient's blood or bone marrow after treatment, even when standard imaging shows no visible disease.
MRD tests use highly sensitive laboratory methods to detect as few as 1 cancer cell among 1 million normal cells. That sensitivity allows oncologists to identify residual disease weeks or months before it becomes clinically detectable, enabling earlier intervention when treatment is most effective.
Terminology: Minimal vs. Measurable
Both terms appear in clinical literature. "Minimal" reflects the tiny quantity of disease; "measurable" emphasizes that modern assays actively quantify—not just detect—residual cancer levels. The European LeukemiaNet (ELN) and the American Society of Hematology (ASH) now prefer "measurable," and NCCN guidelines follow suit.
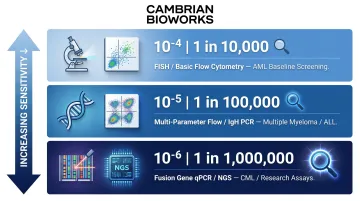
Sensitivity thresholds vary significantly across detection methods—and that variation directly affects which cancers and clinical scenarios each technology suits:
| Sensitivity Level | Detection Limit | Technologies | Typical Applications |
|---|---|---|---|
| 10⁻⁴ (0.01%) | 1 in 10,000 | FISH, basic flow cytometry | AML baseline screening |
| 10⁻⁵ (0.001%) | 1 in 100,000 | Multi-parameter flow, IgH/TCR PCR | Multiple myeloma, ALL |
| 10⁻⁶ (0.0001%) | 1 in 1,000,000 | Fusion gene qPCR, NGS, next-gen flow | CML (BCR::ABL1), research assays |
Tumor-Informed vs. Tumor-Agnostic MRD Tests
Tumor-informed assays (also called tissue-informed) are personalized tests built using a patient's own tumor DNA to create a unique mutation fingerprint. They offer higher specificity and sensitivity—achieving 88% sensitivity in serial surveillance—but require a tissue biopsy upfront and take longer to develop.
Tumor-agnostic assays (tissue-naïve) scan for a broad panel of known cancer-associated mutations without requiring prior tumor tissue. They're faster to run and useful when tissue is unavailable, but sensitivity drops to 59% in serial monitoring, and false-positive risk increases due to clonal hematopoiesis and other confounding signals.
When to use which:
- Tumor-informed: Longitudinal surveillance in patients with available tissue and need for maximum sensitivity
- Tumor-agnostic: Early post-op decision-making, patients without tissue, or when speed matters more than depth
How MRD Testing Helps Monitor Cancer
Treatment Response Monitoring
Serial MRD measurements during chemotherapy, immunotherapy, or targeted therapy reveal whether ctDNA levels are falling (indicating response) or rising (indicating resistance or progression). A 2026 meta-analysis found that unfavorable ctDNA kinetics (rising or persistent ctDNA during treatment) were associated with pooled hazard ratios of 2.6 for overall survival and 2.7 for progression-free survival.
This gives oncologists a real-time signal to adjust treatment plans proactively, rather than waiting for clinical relapse.
Remission Confirmation and Depth Assessment
MRD-negative status (no detectable ctDNA) after treatment correlates strongly with longer progression-free survival. The EVIDENCE meta-analysis evaluated 4,907 newly diagnosed multiple myeloma patients and found that MRD-negative patients had a PFS hazard ratio of 0.40, representing a 60% reduced risk of progression.
That's a level of remission depth confidence that conventional imaging or standard blood tests simply cannot match.
Early Relapse and Recurrence Detection
MRD testing detects molecular signs of cancer recurrence significantly earlier than scans or symptoms:
- Solid tumors broadly: Median lead time of 5.5 months between ctDNA positivity and clinical/radiologic recurrence
- Colorectal cancer specifically: Median lead time of 7.9 months before clinical recurrence
That's more than half a year of actionable warning—time that can be spent initiating salvage therapy when tumor burden is minimal.
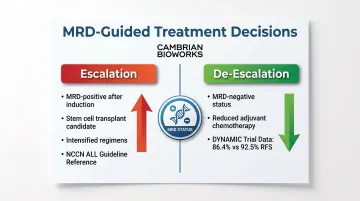
Guiding Treatment Escalation or De-Escalation
MRD status informs risk-stratified decisions in both directions:
- Escalation: Patients persistently MRD-positive after induction therapy may be candidates for stem cell transplant or intensified regimens. NCCN guidelines recommend MRD testing in ALL to guide transplant decisions.
- De-escalation: The randomized DYNAMIC trial in stage II colon cancer showed that ctDNA-guided adjuvant chemotherapy reduced chemotherapy use without compromising recurrence-free survival. Three-year RFS reached 86.4% in ctDNA-positive treated patients vs. 92.5% in ctDNA-negative untreated patients — reducing treatment burden without sacrificing outcomes.
Clinical Trial Utility
MRD status is increasingly used in oncology trials as a surrogate endpoint. The FDA issued final guidance in November 2024 on using ctDNA for early-stage solid tumor drug development and draft guidance in January 2026 endorsing MRD negativity in multiple myeloma as a basis for accelerated approval. In practice, this compresses drug development timelines by years — allowing promising therapies to reach patients faster based on molecular response data rather than long-term survival endpoints.
How MRD Testing Works: From Sample to Result
The entire MRD testing process begins well before the detection technology is applied. The integrity of results depends on decisions made at every stage, from sample collection to data interpretation. Errors or shortcuts in early steps, particularly cfDNA extraction, directly compromise assay sensitivity.
Sample Collection
MRD testing typically uses a liquid biopsy (a blood draw, or bone marrow aspirate for hematologic malignancies). Cell-free DNA (cfDNA) is DNA found in the bloodstream, released from dying cells throughout the body. Circulating tumor DNA (ctDNA) is the subset of cfDNA derived from tumor cells. Blood-based testing is preferred because it's minimally invasive, can be repeated over time, and captures tumor DNA shed from multiple cancer sites simultaneously.
cfDNA Extraction and Processing
That collection quality feeds directly into what happens next. Extracted cfDNA is highly fragile and present in minute quantities, making extraction the most technically demanding stage. cfDNA fragments are typically 120–220 bp long, with tumor-derived fragments often shorter. Poor extraction leads to:
- Low yield
- Genomic DNA contamination (which dilutes the ctDNA signal)
- Degradation of ctDNA fragments
- False-negative results
The numbers make this concrete: sensitivity drops from 82.6% with ≥5 ng cfDNA input to just 46.7% with <2 ng input. In ultra-low ctDNA scenarios, 60% of low-level true positives are missed when using standard 4 mL plasma draws instead of larger volumes. At levels below 0.01%, stochastic sampling becomes the primary cause of false negatives.
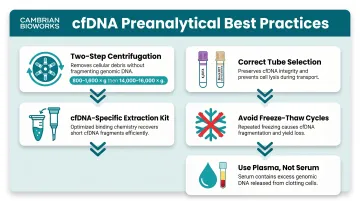
These numbers explain why preanalytical protocols are non-negotiable. Preanalytical best practices include:
- Two-step centrifugation (first 800–1,600 g for 20 min; second 14,000–16,000 g for 10–20 min)
- K₂EDTA tubes (or Streck BCT if processing is delayed >2 hours)
- cfDNA-specific extraction kits (not general DNA isolation kits)
- Avoid freeze-thaw cycles
- Plasma preferred over serum (serum has ~10× more DNA, mostly from WBC lysis)
Cambrian Bioworks' automated cfDNA extraction solutions—including the OncoSeek cfDNA Extraction Kit and the Manta extraction platform—are designed specifically to maximize yield, minimize contamination, and deliver reproducible extraction quality for clinical MRD workflows. Manta holds the CE-IVD mark for clinical DNA extraction, and Cambrian holds ISO 13485 certification and CDSCO IVD certification, credentials that matter when labs need validated, audit-ready extraction solutions.
Library Preparation and Sequencing or Assay Application
Extracted cfDNA undergoes library preparation before analysis by the chosen detection method (NGS/deep sequencing, qPCR, or flow cytometry). Key steps include:
- Adapter ligation to fragmented cfDNA
- Incorporation of Unique Molecular Identifiers (UMIs) to tag individual molecules before amplification
- PCR amplification
- Target enrichment (hybrid capture or amplicon-based)
- Duplex consensus sequencing to filter out PCR and sequencing errors
Different MRD tests use different methods depending on cancer type, available tumor profile, and required sensitivity threshold.
Result Interpretation
Results are reported as MRD-positive or MRD-negative, with quantitative ctDNA measurements in some assays. Sensitivity thresholds typically reach 0.01% or lower for most clinical-grade MRD assays. A single result is rarely interpreted in isolation — longitudinal monitoring over time provides far more actionable insight than a one-time test.
Which Cancers Use MRD Monitoring?
Hematologic Malignancies (Established Use)
MRD testing is most clinically validated and guideline-recommended (per NCCN and ESMO) for blood cancers:
| Cancer Type | Primary MRD Method(s) |
|---|---|
| CML | RT-qPCR (BCR::ABL1 fusion) |
| AML | Flow cytometry, RT-qPCR (NPM1, PML::RARA), NGS |
| ALL | Multiparameter flow cytometry, PCR (IgH/TCR), NGS |
| Multiple myeloma | Next-generation flow cytometry, NGS |
| CLL | Flow cytometry, PCR |
Method selection is driven by each cancer's molecular characteristics — PCR targets specific gene fusions in CML, while flow cytometry and NGS offer the sensitivity needed for myeloma and ALL.
Solid Tumors (Emerging Use)
MRD testing using ctDNA-based liquid biopsy is actively being studied across solid tumor types, including:
- Colorectal cancer (post-surgical surveillance via DYNAMIC, GALAXY, PEGASUS, and BESPOKE CRC trials)
- Breast, lung, bladder, and ovarian cancers
Not yet standard of care for most solid tumors, but clinical evidence continues to build — particularly in colorectal cancer, where ctDNA-guided surveillance is moving closest to routine practice.
Limitations by Cancer Type
Not every cancer type sheds sufficient ctDNA into the bloodstream for reliable liquid biopsy-based MRD detection:
| Shedding Category | Cancer Types | Detection Rate (Metastatic) |
|---|---|---|
| High shedding | Bladder, ovarian, lung, colorectal, pancreatic, breast | 75–90% |
| Low shedding | Thyroid, kidney, prostate, brain (glioma) | <50% |
Tumor location, stage, and biology all influence shedding rates. Rapidly proliferating tumors with significant necrosis — such as pancreatic cancer and small cell lung cancer — release more ctDNA into circulation.
Slow-growing tumors with minimal necrosis, such as papillary thyroid and clear cell renal cell carcinoma, release considerably less. For CNS tumors, the blood-brain barrier further restricts ctDNA from reaching the bloodstream.
How Cambrian Bioworks Supports MRD Testing Workflows
For oncology and molecular diagnostics labs running MRD assays, the technical bottleneck is often not the detection platform — it's the upstream extraction workflow.
Inconsistent cfDNA yields, manual pipetting errors, genomic DNA contamination, and slow batch-dependent processes all introduce variability that compromises assay performance and erodes clinical confidence in results.
Cambrian Bioworks is a Bangalore-headquartered biotech company trusted by 67+ labs globally and present in 5+ countries, specializing in compact, automated nucleic acid extraction solutions designed for clinical and research labs. Their products — including the Manta automated extraction platform and the OncoSeek cfDNA Extraction Kit — directly address these upstream extraction challenges in MRD testing.
Key capabilities relevant to MRD workflows:
- ~55-minute end-to-end cfDNA extraction with minimal genomic DNA contamination
- **High yield from small input volumes** (1–4 mL plasma), delivering 5–20× higher cfDNA recovery compared to competitors
- No batching pressure — process 1 to 32 samples per run, enabling single-sample flexibility
- Remote monitoring for real-time oversight and compliance tracking
- CE-IVD mark (Manta), ISO 13485 certification, and CDSCO IVD certification for clinical-grade quality assurance
These capabilities are already in use across leading oncology institutions:
- Tata Memorial Hospital: FFPE kits for clinical cancer research
- ACTREC: Diagnosis, prognosis, and monitoring of blood cancers
- Strand Life Sciences: Genetic disease and biomarker detection via liquid biopsy
Labs looking to reduce extraction variability and improve MRD assay reliability can contact Cambrian Bioworks at connect@cambrianbioworks.com for a workflow consultation.
Frequently Asked Questions
What is an MRD assay?
An MRD assay is a highly sensitive laboratory test designed to detect and/or quantify residual cancer-derived molecular markers (primarily ctDNA) in a patient's blood or bone marrow after treatment, using methods such as PCR, flow cytometry, or NGS.
How is MRD detected?
MRD is detected through three primary methods, with selection depending on cancer type and required sensitivity:
- Flow cytometry: detects abnormal cell surface proteins
- PCR: targets specific genetic mutations or fusion genes
- NGS/deep sequencing: scans for tumor-specific mutation patterns
What cancers use MRD monitoring?
MRD monitoring is guideline-recommended for hematologic malignancies, including ALL, AML, CML, CLL, multiple myeloma, and certain lymphomas. It is increasingly being studied in solid tumors such as colorectal, breast, and lung cancers via ctDNA liquid biopsy.
What happens after a positive MRD result?
A positive MRD result indicates detectable residual cancer. The oncologist will typically consider treatment intensification, a therapy change, stem cell transplant evaluation, or closer monitoring—decisions tailored to cancer type, stage, and clinical context.
What is the minimum sensitivity threshold for MRD analysis?
The required sensitivity (limit of detection) is generally 0.01% of nucleated cells or lower. In diseases like multiple myeloma, an LOD of 0.001% (10⁻⁵) is required, meaning the assay must reliably detect as few as 1 cancer cell in 100,000 to 1,000,000 normal cells.
What are the limitations of MRD testing?
Not all cancers shed sufficient ctDNA for reliable detection, particularly early-stage solid tumors and low-shedding cancers such as thyroid, kidney, prostate, and brain. MRD negativity does not guarantee cure: cancer may persist below the assay's detection limit. Results can also vary across assay platforms, and coverage and lab availability remain inconsistent.