It is estimated that nearly 1.2 crore men in India may be struggling with infertility - a number that has been steadily rising since the 2000s. Yet, for most, the underlying cause remains undiagnosed. The reasons are multifaceted: low awareness, cultural stigma, and outdated diagnostic approaches that fail to uncover the genetic roots of male infertility.
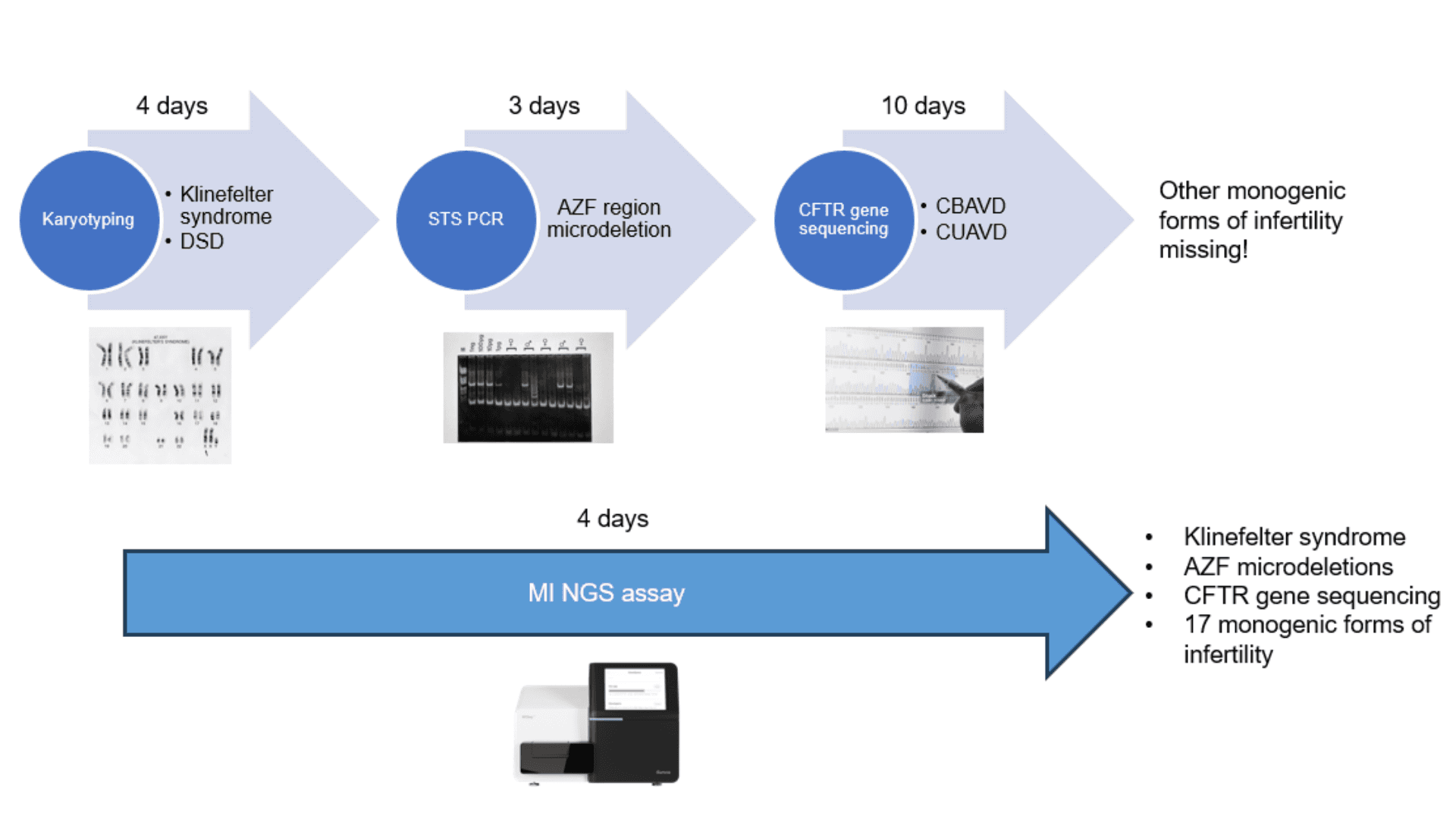
The current diagnostic methods still follow an outdated playbook. For over two decades, standard guidelines have recommended just three tests for men with suspected infertility: karyotyping, Y chromosome microdeletion analysis, and CFTR gene testing. While these can detect broad chromosomal abnormalities or specific deletions, they miss a significant number of single-gene disorders known to cause male infertility. Genes like TEX11, DPY19L2, and AURKC are well-documented in the literature; however, testing for them is rarely done in routine care, largely due to the high cost, technical complexity, and infrastructure required for comprehensive sequencing.
The result is a diagnostic bottleneck: many men with a clear genetic basis for their infertility walk away without answers.
Treatment decisions become less targeted, genetic counseling remains incomplete, and couples are left navigating emotionally and financially taxing journeys without clarity or direction.
A new paradigm emerges from Ahmedabad, India
At the FRIGE Institute of Human Genetics, Dr. Harsh Sheth, with his team of researchers and clinicians, is challenging the status quo. The team developed a targeted NGS panel using single-molecule molecular inversion probes (smMIPs). This panel was designed with a sharp focus: to detect the most clinically relevant genetic causes of male infertility, while keeping turnaround times and costs low.
The panel covers 39 genes, capturing eight key male infertility phenotypes. It also includes coverage for CFTR mutations, Y-chromosome microdeletions, and gonosomal aneuploidies like Klinefelter syndrome, all within a single assay.
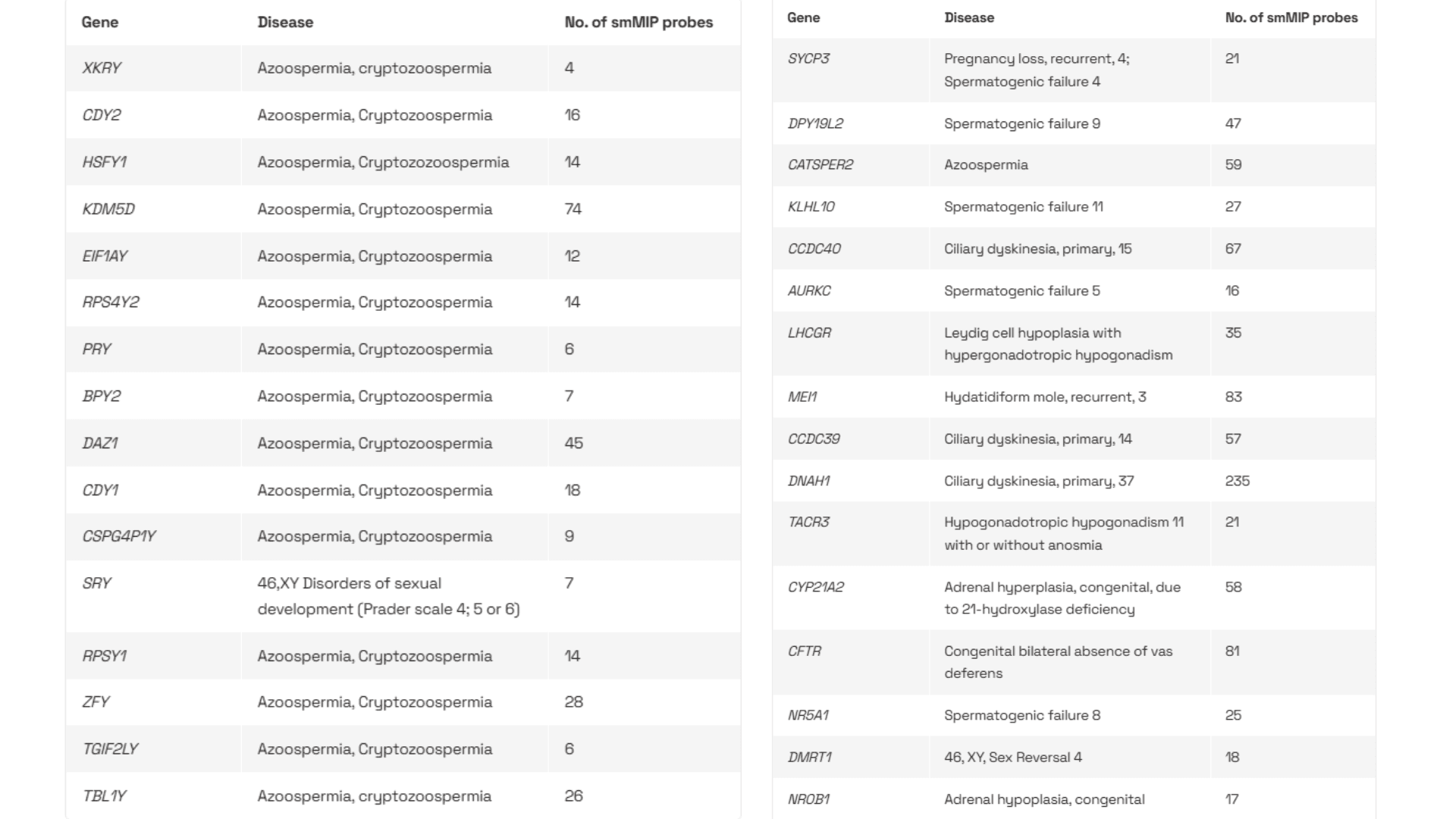

The team employed single-molecule molecular inversion probes (smMIPs), a technology that allows targeted enrichment with high specificity and ultra-low error rates. Each smMIP includes a unique molecular barcode, enabling error correction during sequencing and accurate variant calling even at modest coverage levels.
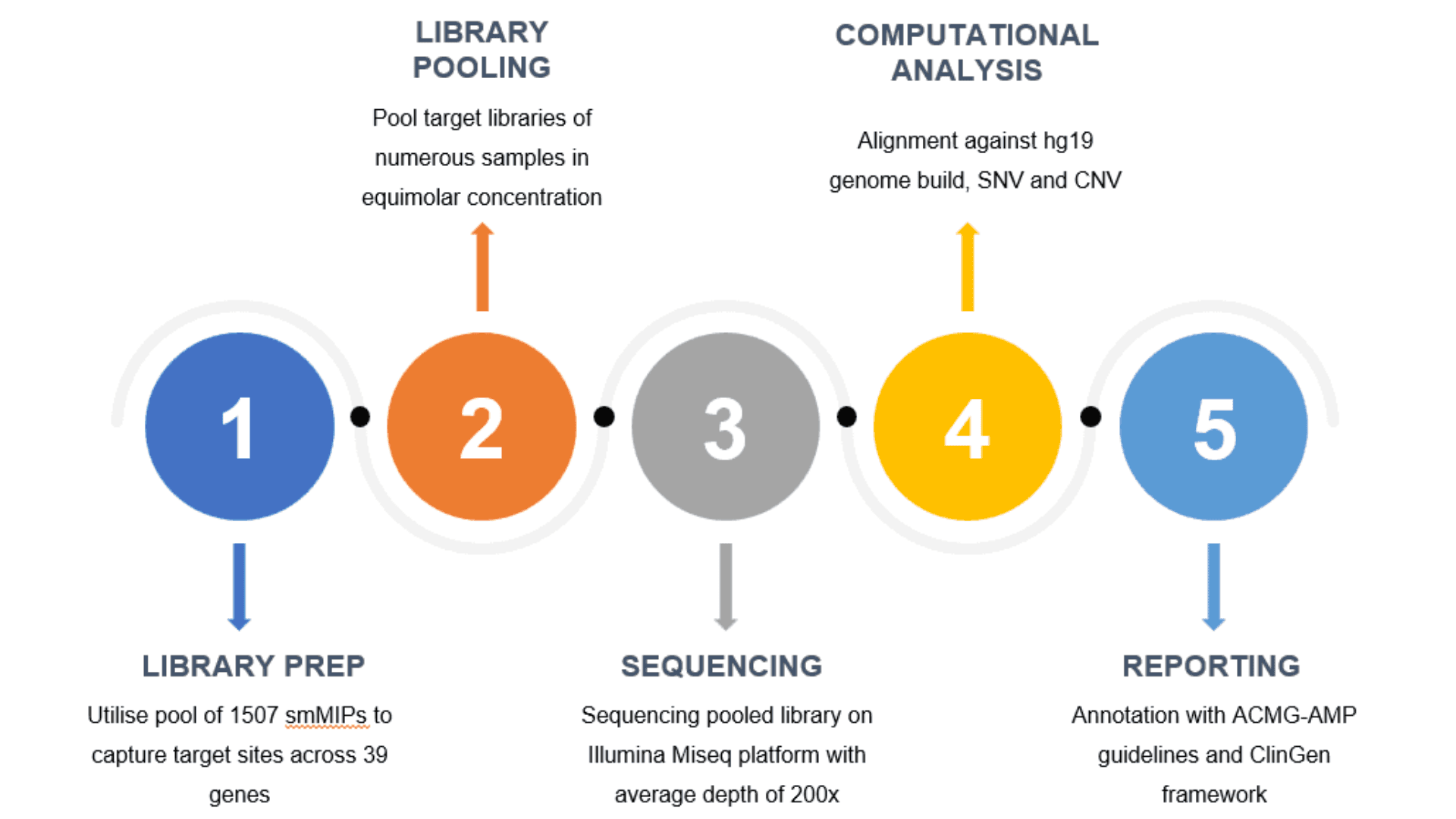
The panel fits perfectly within the throughput of the Illumina MiSeq, a workhorse instrument already common in diagnostic labs across India. It achieves an average sequencing depth of ~200x, more than sufficient for detecting single-nucleotide variants (SNVs), copy number variants (CNVs), and even sex chromosome aneuploidies.
Workflow and technology
The team follows a tightly optimized workflow designed for accuracy and consistency. It begins by extracting DNA from blood samples. At the FRIGE lab, the team uses Manta, Cambrian Bioworks’ automated DNA isolation platform, for extracting high-purity genomic DNA. Manta’s automated process ensures uniformity across runs, which is essential for downstream smMIP-based assays where uneven input DNA can lead to poor coverage and false negatives.
The following table summarizes the QC metrics used by the FRIGE lab and the proportion of samples that met the acceptance criteria for downstream sequencing.
QC Metric | Threshold | Samples Passing (n=120) |
DNA concentration (Nanodrop) | 200–500 ng/µL | 120/120 |
DNA concentration (Qubit) | 100–400 ng/µL | 120/120 |
Library size | 271 bp | 120/120 |
Library concentration | > 10 nM | 120/120 |
Once DNA is extracted, the smMIP-based library preparation is performed. Multiple patient libraries are pooled in equimolar concentrations before sequencing. The data is then processed through a streamlined pipeline that aligns reads to the hg19 genome, calls variants, and annotates them using ACMG-AMP guidelines and the ClinGen framework.
Patient cohort and diagnostic evaluation
A total of 247 men referred for evaluation of infertility were included in the study. The mean age was 34 ± 5 years (range 24–51 years). Among them, 48 participants had a prior history of assisted reproductive technology (ART), and 13 reported a family history of infertility.
Primary clinical phenotypes at presentation:
Phenotype | n | % |
Oligoasthenoteratozoospermia (OAT) | 124 | 50.2% |
Azoospermia | 79 | 31.9% |
Oligozoospermia | 5 | 2.0% |
Qualitative spermatogenic defects* | 39 | 15.8% |
Total | 247 | 100% |
*Isolated qualitative abnormalities such as asthenozoospermia or teratozoospermia without marked oligozoospermia
Conventional Testing vs smMIP-Based Sequencing
All participants underwent the standard first-line genetic workup, including karyotyping and Y-chromosome (AZF) microdeletion analysis, which together form the current diagnostic guideline for male infertility.
A subset of patients, for whom no abnormalities were detected through these tests, underwent further evaluation using next-generation sequencing, either through the targeted smMIP panel or whole-exome sequencing (WES).
Summary of diagnostic yield:
Test methodology | Patients tested (n) | Diagnostic yield | Notes |
Karyotyping | 247 | 1.21% (3/247) | Detected large chromosomal abnormalities |
AZF microdeletion testing | 247 | 9.7% (24/247) | Detected Y-chromosome deletions |
smMIP targeted sequencing panel | 120 | 5.8% (7/120) | Excluded patients with AZF deletions or aneuploidies |
Whole-exome sequencing (WES) | 48 | 8.3% (4/48) | Subset not tested by smMIP panel |
The smMIP panel provided a molecular diagnosis in seven patients who had tested negative by conventional approaches.
Among these:
4 cases (57%) carried biallelic CFTR variants,
1 case each harbored pathogenic mutations in DNAH1, NR5A1, and KLHL10, all well-established genes implicated in male infertility.
When combined, sequencing-based methods (smMIP + WES) increased the overall diagnostic yield by ~6–8% beyond the standard karyotype + Y-deletion testing, providing additional genetic clarity in cases that would otherwise remain unexplained.
The new benchmark
The entire turnaround time, from DNA extraction to final report, is completed in under four days. This is a significant improvement over traditional multi-step testing approaches, which can take 10 days or more. It marks a shift from fragmented, reactive diagnostics to an integrated, proactive genomic care model.
The team has also paid close attention to the economic feasibility of this process. The full cost of the assay, including extraction, library prep, sequencing, and analysis, falls between $120 - $130 per sample. This makes it one of the most affordable, high-accuracy genetic tests for male infertility currently available, especially when compared to international benchmarks or multi-test workflows.
The FRIGE’s smMIP-based workflow sets a new benchmark in reproductive genomics, uniting scalability, affordability, and rigor. It delivers a reliable, rapid, and cost-effective pipeline ready for deployment across diagnostic labs in India.
As Dr. Harsh Sheth summarises,
When you add a focused smMIP panel to the standard workup, you stop losing the monogenic cases, clearer answers at a cost and turnaround time that fit routine diagnostics.
Continue reading…